Update May 29th: Jewish Family Services which initially resettled the Muslim Somalis says it will work to rectify the situation, here.
Mayor: “No mas, no more!”
Wyomingare you listening! Does anyone wonder anymore how “pockets of resistance” are building to this program that is overloading your cities and towns with impoverished third-worlders?
Somali family (father, two women, 12 kids) relocated from roach-infested house with no electricity! The two women are said to be sisters—Ha! Ha!
SPRINGFIELD – City officials said Tuesday that Somali refugees including 12 children were found living in deplorable conditions in a Union Street apartment that had a heavy infestation of roaches and no electricity.
The duplex apartment at 515 Union St. was condemned Thursday by the city, and the tenants — believed to number three adults and 12 children — were relocated after Code Enforcement and Housing officials were notified and conducted the inspection, city officials said.
“It was the heaviest infestation of roaches I have seen in years,” said David Cotter, the city’s deputy director of code enforcement in the Housing Division. “They were all over the walls, floors, ceilings, window areas, doorways. I ordered all the inspectors out of there until we could get a full extermination report.”
According to police, one child was doing her homework outside the building under a street lamp on Wednesday night due to the lack of electricity, Cotter said.
Mayor renews call for a halt to any new resettlement in Springfield. The only way to get the attention of the State Department and the arrogant contractors is to make a huge publicity stink, so readers, help Springfield by spreading this news far and wide across America!
Mayor Domenic J. Sarno, who has been critical of the refugee resettlement policies in Springfield in the past, renewed his criticism on Tuesday. Refugees have not received adequate follow-up services from the resettlement agencies, from the federal level on down, leaving them to be a strain on city services, Sarno said.
“Where is the accountability?” Sarno said.
The residents were living in poverty and in crowded, unsafe conditions, Sarno said.
Sarno had urged the federal government to stop locating new refugees in Springfield last year, and called for a moratorium again on Tuesday.
“No mas, no more,” Sarno said.
Contractors are surely saying among themselves, but wouldn’t dare say so publicly at this moment: NOT our problem, we were only responsible for them for up to 8 months in 2003! Surely even the bureaucrats at the US State Department and the Office of Refugee Resettlement (in HHS) are saying—people don’t understand, it’s not our job to take care of refugees for years. But, you know what! Whose fault is that that the public doesn’t understand the program?
The complexity and secrecy surrounding refugee resettlement in the US for over three decades now has shielded the federal program from public understanding and scrutiny—until now that is!
Wandering Somalis!
Robert Marmor, president and chief executive officer of the Jewish Family Service of Western Mass., said his agency resettled the initial family in Springfield in September 2003.
The family later moved to Nashville, Tenn., and then returned to Springfield in 2008, and asked for and received assisted then, Marmor said. The family then moved to Utica, N.Y., in 2011, before returning to Springfield, he said.
In Minnesota, 63% of Somalis live in poverty and I will bet in every state where they are congregated a similar statistic is available.
By the way, Mayor Sarno is a Democrat and the irony is that it was none other than the former Senator from Massachusetts—‘Don’t bring-em to Hyannis’ Kennedy who is ultimately responsible for the mess now in Springfield.
Ted Kennedy, Joe Biden and Jimmy Carter brought us the Refugee Act of 1980 and the present system that doles out your tax dollars to unaccountable “non-profit” contractors to drop off the refugees in overloaded cities, care for them for a few months and then walk away.
Our complete archive on Springfield, Mass is here.
Massachusetts is a ‘Wilson-Fish’ state and the program may ultimately be found to be illegally administered.
If you have read this post on May 28th and are infuriated, take a few minutes and write to the US State Department by tomorrow (Thursday) 5 p.m. Go here for more!
Editors note: One of the primary purposes of RRW is to educate readers about how the complex Refugee Resettlement program of the US State Department and the US Department of Health and Human Services (Office of Refugee Resettlement) works. When you have some basic understanding of how it operates (and how it may have been changed from its original legislative intent) you will be much more effective in demanding accountability for the taxpayers of your state and others (including the refugees!) who will be impacted by the program.
This is a states’ rights issue!
If you live in one of the following 11 states you should be paying close attention to how the program is run in your state and begin questioning whether the federal government has the constitutional authority to pass off a federal program to a non-profit group which effectively eliminates, or nearly eliminates, any state control of how state tax dollars are spent.
Do you live in one of these Wilson-Fish states?
Alabama, Alaska, Colorado, Idaho, Kentucky, Louisiana, Massachusetts, North Dakota, South Dakota, Tennessee or Vermont.
***Update*** There are 12 W-F states at this time (Oct. 2015): Alabama, Alaska, Colorado, Idaho, Kentucky, Louisiana, Massachusetts, Nevada, North Dakota, South Dakota, Tennessee and Vermont
A grassroots volunteer has prepared this important Frequently Asked Questions (FAQ) and answers about the federal Wilson-Fish program.
Holly Johnson (TN Catholic Charities) left, and Jan Reeves (Idaho Mountain States Group) right, call the shots on refugee resettlement in their Wilson-Fish states. http://www.isedsolutions.org/blog/wilson-fish/wf-workshop-highlights
What is Wilson-Fish?
There are 3 ways in which the federal government disburses the 8 months of federal refugee cash assistance (RCA) and refugee medical assistance (RMA) funds to eligible refugees.(1) These funds are disbursed through:
• a state administered program, or,
• a public-private partnership program, or
• a Wilson-Fish “alternative” program
The Wilson-Fish alternative (so named for its Congressional sponsors) was added in 1984 as an amendment to the Immigration and Nationality Act. The amendment authorized the Secretary of Health and Human Services to implement alternative projects for refugees:
“[t]he Secretary shall develop and implement alternative projects for refugees who have been in the United States less than thirty-six months, under which refugees are provided interim support, medical services, support services, and case management, as needed, in a manner that encourages self-sufficiency, reduces welfare dependency, and fosters greater coordination among the resettlement agencies and service providers.”
The Wilson-Fish amendment was initially introduced as part of the FY1985 Continuing Resolution on Appropriations. On October 2, 1984 when Senator Wilson introduced Amendment No. 6965, he stated very clearly that:
“The specific intention of this amendment is to encourage refugee self-support and employment in California, a State which consistently receives at least 22 percent of all incoming refugees. A disproportionate number of refugees end up on welfare rolls. The language in this amendment will allow alternative approaches to this welfare dependency cycle.” (emphasis added)
In contrast to the “specific intent” of the Wilson-Fish amendment, the U.S. Office of Refugee Resettlement has unilaterally and without legislative authorization, used the Wilson-Fish alternative to continue resettling refugees in states where the State has decided to discontinue participating in this non-mandatory federal program.
For example, the 1995 notice of available funding for Wilson-Fish projects states that “This announcement [for funding Wilson-Fish projects] also provides for an alternative project to be a vehicle to continue resettlement programs in States where the State government chooses not to administer RCA/RMA or equivalent programs.”
The U.S Office of Refugee Resettlement website states that “the purposes of the Wilson-Fish program are to:
~Increase refugee prospects for early employment and self-sufficiency
~Promote coordination among voluntary resettlement agencies and service providers
~Ensure that refugee assistance programs exist in every state where refugees are resettled”
The last “purpose” added by the federal agency, is not supported by either the language or intent of the Wilson-Fish statutory language.
Why did Congress feel there was a need to add an alternative program like Wilson-Fish?
Sen. Pete Wilson from California was the Senate sponsor of the Wilson-Fish amendment. When he introduced the amendment he stated very clearly his concern about the high rate of refugee welfare dependency, combined with the high number of refugees being resettled in his state.
His concerns were well founded. Center for Immigration Studies fellow, Don Barnett who has been researching and writing about issues related to refugee resettlement notes that:
“According to the latest data available, a federal study of refugees who have been in the country 5 years or less, the unemployment rate for refugees was 21 percent compared with 9 percent for the U.S. population in 2010. Twenty-six percent were dependent on cash assistance, 63 percent were in the food stamp program and 48 percent were in Medicaid or short-term federal Refugee Medical Assistance. The federal welfare program SSI is a good indicator of long-term welfare dependency rates. It is generally a lifetime entitlement and usually includes Medicaid and other social services. The federal study of arrivals over the previous five years found an 11.6 percent rate of usage – about 2.5 times the national average.
Most of this cost is borne by the federal taxpayer, but programs such as Medicaid have state cost components as well.”
How do states decide if they want to be a Wilson-Fish state?
The U.S. Office for Refugee Resettlement receives the application and decides. The scope of services available to refugees from a Wilson-Fish program is similar to that of the State-Administered Refugee Resettlement Programs, which in turn is similar to regular domestic public assistance programs. States, voluntary resettlement agencies, and other nonprofit refugee resettlement organizations may apply to initiate a Wilson-Fish program.
In several states, the State decided to withdraw from the federal refugee resettlement program. Thereafter, the U.S. Office for Refugee Resettlement (ORR) selected a refugee resettlement agency to operate as the “state designee” for purposes of receiving and disbursing federal funds to refugees who are not eligible for state Medicaid and cash welfare programs. In these states, the resettlement agency applied directly to the ORR to operate a Wilson-Fish project.
For example, data from Tennessee shows that once the state withdrew from the program and the federal contractor took over operating the program, resettlement numbers increased by approximately 66%. Why? The 2012 U.S. General Accounting Office report “Greater Consultation with Community Stakeholders Could Strengthen Program” documented the major contributing factor:
“Because refugees are generally placed in communities where national voluntary agency affiliates [local offices] have been successful in resettling refugees, the same communities are often asked to absorb refugees year after year. One state refugee coordinator noted that local affiliate funding is based on the number of refugees they serve, so affiliates have an incentive to maintain or increase the number of refugees they resettle each year rather than allowing the number to decrease.” (emphasis added)
Which states currently operate as Wilson-Fish?
Wilson-Fish programs are currently operating in:
~Colorado, Massachusetts and Vermont but the State government still runs the program
~North and South Dakota – State has withdrawn; Lutheran Social Services runs the program
~Idaho – State has withdrawn; Mountain States Group runs the program
~Alabama, Alaska, Kentucky, Tennessee, Louisiana (only partial withdrawal) – State has withdrawn; Catholic Charities runs the program
The parent organization of Lutheran Social Services is Lutheran Immigration and Refugee Services, one of the big 9 resettlement agencies that contracts with the federal government. In 2011, their total reported revenue was $31,653,748 of which $30,376,568 (96%) was taxpayer money. Their CEO was paid $204, 186 in salary and benefits.
The parent organization of Catholic Charities is the US Conference of Catholic Bishops which is the largest of all the federal refugee resettlement contractors. Their 2011 reported revenue $72,102,484 included $66,723,452, which is approximately 93%, from federal funding.
Does the U.S. Office of Refugee Resettlement or the Dept. of Health and Human Services have the authority under the Wilson-Fish amendment to fund a non-profit organization and continue a resettlement program in a state when that State has withdrawn from the federal program?
The Wilson-Fish amendment did not address this issue specifically. All the amendment language did was allow for the establishment of “alternative projects” designed to accomplish the specifically stated goals of establishing a program that “encourages self-sufficiency, reduces welfare dependency, and fosters greater coordination among the resettlement agencies and service providers.”
While the Secretary of the federal agencies must implement the objectives of the authorizing legislation, there is no language in the Wilson-Fish amendment that permits a federal agency to circumvent a state’s decision to withdraw from the federal program by funding a private non-profit organization to establish or continue the program in lieu of the state.
This issue is particularly relevant because of the federal government deliberately shifting the cost of its program to the states, and the utilization of state-funded resources to address long-term needs of refugees.
Funding announcements for Wilson-Fish projects identify two categories of Wilson-Fish projects: those to “establish or maintain a refugee program” in a State that has either withdrawn from all or part of the refugee program, and projects that provide an “alternative to the existing system” of providing for refugees.
Only this last category of project was intended and contemplated by the Wilson-Fish statutory amendment.
Despite this limitation and the fact that the 1995 funding notice, for example, reflected the intent of the Wilson-Fish amendment to “encourage alternative projects in areas where refugees have had a history of extended welfare utilization,” this notice and subsequent ones also state that funding for Wilson-Fish projects are a “vehicle to continue resettlement programs in States where the State government chooses not to administer RCA/RMA or equivalent programs.”
What happens to the mandated consultation process between resettlement agencies and state and local governments when a state withdraws from the federal program and a federal contractor is permitted to use Wilson-Fish as a “vehicle to continue [the] resettlement program”?
The Wilson-Fish State Refugee Coordinator position is paid as part of the federal grant meaning that the “state coordinator” is actually a federal contractor, not a state-paid employee. So if the state government has withdrawn from the federal program, the federal contractor running the program is no longer accountable to the state’s taxpayers or the state and local governments.
Tennessee is a good example.
The Tennessee state government withdrew from the refugee resettlement program in late 2008. The U.S. Office of Refugee Resettlement (ORR) thereafter contracted with refugee resettlement agency Catholic Charities of Tennessee (CCTN) to operate as the “state designee” to disburse federal funds. CCTN then applied to ORR and was granted permission to operate as a Wilson-Fish. CCTN then set up a separate office called Tennessee Office for Refugees (TOR) as a separate department of CCTN. TOR would run the federal program for the state.
Under the Tennessee Wilson-Fish project, the required consultation and any monitoring of refugee resettlement activities in the state, is internal to Catholic Charities and the other resettlement agencies operating in the state. As described by CCTN, their Director of Refugee Resettlement consults with the TOR state refugee coordinator who also works for Catholic Charities. Consult with the state refugee health coordinator who also works for CCTN and who also reports to the same agency’s TOR state refugee coordinator is an internal process highly vulnerable to conflicts of interest. Nor does this closed, self-serving system lend itself to any objective or independent compliance monitoring.
CCTN’s annual reports show that its largest program is the Tennessee Office for Refugees – TOR. CCTN’s second largest program is its own refugee resettlement program which receives funding from TOR.
A 2011 report issued by the Migration Policy Institute, a refugee advocacy organization, claims that after the consultation process, all proposed resettlement plans are provided to ORR and states. “If a state opposes the plan, PRM [the federal agency] will not approve it.” The U.S. Senate Committee on Foreign Relations recommended that in the case of a disagreement among stakeholders over resettlement, the “state refugee coordinator should be able to request a moratorium for the community.”
Under what circumstances would a Wilson-Fish “state” refugee coordinator (who is a federal contractor), working in concert with the other federal contractor refugee resettlement agencies that earn their funding for each individual refugee they resettle, oppose a plan? Maybe if the numbers were too low? Requesting a moratorium would be a conflict of interest for a Wilson-Fish state refugee coordinator.
Following the pattern of what happens when refugee resettlement is privatized, TOR’s 2011 Wilson-Fish application detailed a plan to expand refugee resettlement in Tennessee by adding two new refugee resettlement agencies and by increasing the number of refugees brought to the state.
Are refugees served under a Wilson-Fish project allowed to enroll in Medicaid or receive TANF (Temporary Assistance for Needy Families, aka, cash welfare)?
The statutory language of the Wilson-Fish amendment states that:
“Refugees covered under such alternative projects shall be precluded from receiving cash or medical assistance under any other paragraph of this subsection or under title XIX or part A of title IV of the Social Security Act [42 U.S.C. 1396 et seq. 601 et seq.]”
Title XIX refers to Medicaid and part A of title IV refers to TANF (cash welfare).
The Wilson-Fish amendment was intended to address welfare dependency. The U.S. Office of Refugee Resettlement has qualified the original language and intent of the Wilson-Fish amendment. The funding announcement notes that only when an application for an alternative Wilson-Fish project includes “alternative medical assistance” will the recipient be precluded from using Medicaid despite the statutory language.
When the Wilson-Fish amendment was introduced on October 2, 1984, Sens. Weicker and Proxmire both confirmed that the language of the amendment was “budget neutral” meaning that the amendment allowing for the alternative projects added no additional funds to the appropriations bill under consideration. Since there was no separate appropriation for Wilson-Fish projects, funding would be drawn instead from funds otherwise earmarked for refugee cash and medical assistance (RCA and RMA) and social services allocations for the State-administered program.
Refugees are only permitted to use either Medicaid or the 8 month federal refugee medical assistance (RMA) – they cannot get both. And they either get TANF or refugee cash assistance (RCA) – they cannot get both.
Since the Wilson-Fish projects are funded with the RMA and RCA funds, refugees served under a Wilson-Fish project cannot also utilize Medicaid and TANF – it would be redundant funding.
Medicaid expansion is particularly relevant to where federal contractors are looking to increase refugee placement. That’s because under Obamacare, states were given the option to make Medicaid available to groups not currently eligible for it. This could include, for example, lowering the income eligibility. And because many refugees start out in lower or minimum wage jobs, more could potentially qualify for Medicaid.
The 2014 Dept. of Health and Human Services briefing titled “Key Indicators for Refugee Placement” included information about which states have expanded or are considering expanding Medicaid under Obamacare:
“One major factor that may affect placement is the implementation of the Affordable Care Act (ACA). Accordingly, this year’s data has incorporated information on health access determinants including updates on states that plan to expand Medicaid during the final implementation phase of ACA, and states that have ruled Medicaid expansion out.”
Refugee contractors have publicly stated that they will focus more and more of the future refugees placements in those states where there is Medicaid expansion.
_________
Footnote from paragraph one: (1) Only refugees who are NOT eligible for their state’s Medicaid program can receive the 8 months of federal medical assistance funds. The federal money stops if a refugee becomes eligible for their state’s Medicaid program even if the full 8 months have not elapsed.
Editor: Note that this post is archived in our category ‘where to find information.‘ Check it out if you are trying to educate yourself on refugee resettlement and immigration generally. And, don’t forget to see our fact sheet which every day recently has been our top post (follow top posts in our right hand sidebar)!
One of the first things a “welcoming” community in America becomes aware of is the cost of refugee health care at a county health department.
We first became aware of how quickly “pockets of resistance” grow locally when a health department is overloaded with refugee vaccination needs and medical treatment costs for such diseases as TB and HIV/AIDS. Here is one of our earliest posts on the problem in Ft. Wayne, Indiana (2007!).
Now we see that the US State Department and the CDC are going to try to get a greater number of refugees vaccinated abroad before they enter the US. It sounds like a good move for medical reasons. But, it also provides a fig leaf by shifting the cost from one group of taxpayers to the other. While relieving the burden on local and state taxpayers, the costs will be borne by the federal taxpayers, so what is the difference!
Wyoming please note that if they are successful in vaccinating 56% abroad (we resettle on average 70,000 a year), that still leaves 30,800 or so refugees whose vaccination needs will be paid for by state and county taxpayers along with many other of their medical needs! Wyoming Governor Matt Mead thinks the refugee program is free to Wyoming and that the federal government has a money tree!
The refugees have agreed to participate in a vaccination project that will introduce multiple vaccines overseas, depending on age, before they arrive to the US. The project is a partnership between CDC’s Division of Global Migration and the US Department of State’s Bureau of Population, Refugees, and Migration (PRM). CDC and PRM are co-funding this project for approved refugee applicants in the US Refugee Admissions Program (USRAP).The goal of the project is to provide cost-effective public health interventions, improve refugee health, and limit the number of vaccinations refugees will need after they arrive in the US. In addition to Kenya, the vaccination project is being implemented by IOM with USRAP in Ethiopia, Thailand, Malaysia, and Nepal.
[….]
This project has been implemented in five countries and will provide vaccinations overseas to 56 percent of US-bound refugees each year, saving state and local health departments from the cost and time to provide those vaccines after the refugees reach their new homes in the US.
And thereby eliminating an important driver of community resistance to refugee placement.
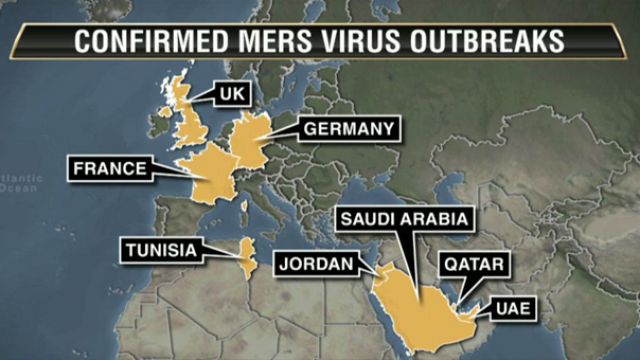
Another Saudi national has brought a case of the deadly MERS virus to America. This story has been all over the national and local news since it broke two days ago.
The US will now have to be added to the map. Where else?
As we have said on previous occasions, if Americans don’t wise up to the security threats, the cultural challenges, the expense to taxpayers of opening our borders to the world, the one thing that will get their attention is the threat of deadly diseases their kids might contract at school, or they might pick up in a hospital or on the subway.
MERS is making the national news, but others, especially tuberculosis, are on the rise in the US immigrant population and the cases are reported only in the local media. See our Health issues category for more.
ORLANDO, Fla. (AP) — Employees at two Orlando hospitals who came in contact with a Saudi resident infected by the second confirmed U.S. case of a rare virus are being monitored for symptoms and have been told to stay home for two weeks, health officials said Tuesday.
Fifteen hospital workers at Dr. Phillips Hospital and another five employees at Orlando Regional Medical Center were being monitored at home for fever, chills and muscle aches, said Dr. Antonio Crespo, an official with the hospital system.
So far, none of them has tested positive for MERS, or Middle East Respiratory Syndrome. MERS is a respiratory illness that begins with flu-like fever and cough but can lead to shortness of breath, pneumonia and death.
The Saudi resident was being treated at Dr. Phillips Hospital, where he showed up at the emergency room May 8. Three days earlier, he had visited Orlando Regional Medical Center with a friend who went to the hospital for a test.
Two workers at Dr. Phillips Hospital, who were not identified, have shown flu-like symptoms recent days. One of them was sent home, and the other has been hospitalized in isolation. Both are awaiting test results that could come later this week. Crespo said MERS has been shown to have a 14-day incubation period.
[….]
The White House said Tuesday that President Barack Obama had been briefed on the MERS cases in the U.S.
We would be so much better off as a nation without the Saudis money, oil, students and diseases!
Affordable Care Actnavigators have managed to sign up large numbers of immigrants in a health care plan, but mostly because the language barrier is so great, those same counselors now need to be sure those who signed use their insurance and PAY THEIR BILL.
Burmese refugee surprise: I have to pay even if I’m not sick???
One of the counselors said you could be here for 20 years and speak perfect English and still not be able to figure it out!
When Biak Sung escaped from Myanmar in 2011, there was no health insurance for people like her.
So it’s not surprising that months after buying a plan on the Affordable Care Act marketplace, Sung, 27, a mother of two and a political refugee – whose English consists of “hello” and “thank you” – doesn’t know how to use her family’s policy.
Last week, Sung, whose husband works full time, went to the Southeast Asian Mutual Assistance Association Coalition (SEAMAAC) in South Philadelphia to learn about her new policy, an Independence Blue Cross silver-tier Keystone HMO Proactive plan.
“She doesn’t know what steps to do next and she is concerned,” said Zing Thluai, a SEAMAAC worker who speaks one of three Burmese dialects.
Navigators/counselors now going back to make sure they pay their bills!
So the staff started calling clients, asking whether they had paid their premiums or needed assistance. It wasn’t unusual to hear people say they had received a bill but didn’t know what to do with it because they weren’t sick. Staffers had to explain that the bill must be paid every month, sick or not.
This is surely the next shoe to drop on Obamacare—getting the cash out of people who signed up (and not just the immigrants)!
See our extensive ‘Health issues’ category for more on refugee health.