Washington has had a slight decline in tuberculosis (TB) cases in 2014 but state and local public health officials are still on high alert when it comes to this disease. TB is second only to HIV/AIDS as the greatest infectious killer worldwide.
[….]
“Tuberculosis remains a disease of concern internationally and in Washington,” State Communicable Disease Epidemiologist Dr. Scott Lindquist said. “TB can be diagnosed, treated, and cured, yet it takes real commitment and effort to effectively deal with this disease.”
[….]
Drug-resistant TB continues to be a serious public health threat in Washington. This variation requires longer treatment periods with drugs that are more expensive. In 2014, 20 cases reported to the state health department were resistant to one or more drugs currently used as a first line of treatment for TB; two were multi-drug resistant. Infection control procedures must be in place in hospitals or health care settings to prevent exposure to this disease and keep it from spreading.
TB rates are often higher among racial and ethnic groups. In 2014, 72.5 percent of cases in the state were in people born outside the U.S. or its territories. In 2014, 43.5 percent of all cases in Washington were among Asians, followed by Hispanics (15.5 percent), blacks (15.5 percent), and whites (11.9 percent). Between 2012 and 2014 the greatest risk of TB in Washington was among Native Hawaiian and Other Pacific Islander communities (27.7 cases per 100,000).
27 students and teachers have tested positive for TB in one Kansas City, MO high school. No word on who Patient Zero might be, see the story here.
See our health issues category, here, for more on refugee physical and mental health problems.
This is a little story I didn’t get around to a couple of days ago. Thanks to Robin (and maybe someone else) who sent it my way.
We think we have it bad—check out Germany’s measles cases and this more detailed story. Spikes in Germany related to refugee and asylum seeker waves. http://www.digitaljournal.com/life/health/measles-outbreak-in-germany-10-times-worse-that-in-usa/article/425487?noredir=1
Authorities in Berlin say a spike in measles infections has been traced to unvaccinated refugees but at least two measles cases appear to have come from the United States.
Berlin has recorded 468 cases of measles this year, more than the rest of Germany had during all of 2014.
Dr. Dirk Werber of Berlin’s state health office said Friday that a child asylum seeker from Bosnia is considered the index case because many subsequent infections among refugees were genetically identical.
Measles has since spread to Berlin’s non-refugee population, partly because immunization rates among over-45s are low.
Two cases are believed to have been caught in the US. Related to refugees here too? That we don’t know.
Werber said one woman and possibly a child appeared to have contracted measles while traveling in the United States.
Germany is having its migrant problems, that is for sure! Click here for our complete archive on Germany.
I like this photo of Gov. LePage holding the Heritage Foundation’s copy of the US Constitution.
Update!Reader Dana sent us this link. 16 Test positive for TB at Sacramento area high school—wonder where it came from???
Not physically slapped around, but verbally in the Bangor Daily News which apparently wants to debunk his claim. Note the first sentence of the story by Christopher Cousins—if you don’t read beyond that, you have been told what the media wants you to believe.
….however, there are a large number of ACTIVE TB cases in Maine!
Regular readers may remember that Maine has become the go-to state for asylum seekers—migrants who got into the country one way or another and are now seeking ‘refugee’ status. In Maine, while they are waiting for the decision, they can get various social services that are not available elsewhere.
There may be other states that give out welfare to asylum seekers, but I haven’t read about those. Gov. LePage has been attempting to remove the sweetener that Maine has been providing.
AUGUSTA, Maine — The consensus among public health experts regarding Gov. Paul LePage’s comments linking illegal immigrants to the spread of infectious diseases during his State of the State address on Tuesday is that they have seen no data to back up his claims.
Officials from the LePage administration have provided no substantiation for the comments and have not responded since Wednesday to the Bangor Daily News’ requests for data and comment on the matter.
Here’s what the governor said:
“When a refugee comes here from a foreign country, they get a medical assessment, and we know their health. But when they come here illegally, they don’t get medical assessments. And one thing that we don’t want to see is the uptick of hepatitis C, HIV and tuberculosis. But it is here. We are dealing with it. And it is very costly. So if nothing else, they should be getting a medical assessment when they get here.”
By the way, even if a refugee gets a medical assessment before entering the US, the presence of TB or HIV is not a bar to entry.
So, after many paragraphs of making light of the governor’s comments we come to this one (below) on TB. I was blown away by the number of ACTIVE Tuberculosis cases diagnosed in Maine. Do you remember when one guy with active TB got on a plane somewhere a few years ago and all hell broke loose in the media — well, heck, why isn’t there a lot of news about these ACTIVE cases in Maine? How many are there in other states?
The resettlement industry mouthpieces are quick to tell us that LATENT TB is no big deal. O.K. but what about all these active cases getting in here? Twenty plus cases of ACTIVE TB over three years is a lot of cases—and, you are paying for their meds!
Active tuberculosis cases were higher in 2012 and 2013 than they had been since 2009, with 15 reported cases in 2013. There were less than 10 new cases reported in 2014, according to Hannan’s data. The CDC also tracks latent cases, which means the tuberculosis bacteria is present but the patient shows no symptoms (untreated latent tuberculosis is a precursor to full-blown tuberculosis in up to 10 percent of cases). There were 433 latent cases recorded in 2013, up from 398 in 2012. The CDC report also includes the country of birth for people recorded to have latent tuberculosis. The top countries of origin for latent tuberculosis cases were Angola (41), Burundi (43), Congo (51), Iraq (41), Rwanda (38), Somalia (53) and the United States (78).The 2013 CDC report contains no information about how long the patients had been in Maine before their diagnosis.
See our‘health issues’category for more on diseases, mental health problems and other medical issues involving refugees. I’ve often said that health concerns are going to have a far greater impact on American attitudes toward immigration than the fear of terrorists getting in here.
Since I was on the subject of refugee health and university professors in my last post, here is a story from Canada (one of few stories not discussing Islamic terrorism and immigration!).
By the way, if you didn’t know, the US refugee program admits refugees with HIV and we supply their meds in your local health departments. I had forgotten, but we have a fairly large archive on HIV and refugees, click hereto learn more.
Renu Mandhane, the program director International Human Rights Program at the U of Toronto: Canada should provide asylum and medical care to HIV positive refugees.
Canadian refugee and resettlement policies are negatively affecting would-be refugee claimants abroad who have HIV or are at high risk of contracting the virus, a University of Toronto program has alleged.
The International Human Rights Program at the university’s faculty of law is launching a research project to advocate for changes on the immigration policy that has created the “designated countries of origin” list.
[….]
“Having HIV when you’re a refugee living in a camp bordering Syria is potentially a death sentence,” she said. “Canada can play an important role in the global fight against HIV by providing asylum to people affected or at high risk, and provide them with access to medical treatment.”
The research project will focus on Mexico and Syria as case studies. Syria is not on the list of countries deemed to be safe, but there are many refugees on its borders that need equal attention due to the vulnerability surrounding them, said Mandhane.
[….]
The program, which recently got a $75,000 grant from Elton John AIDS Foundation, is expected to conduct field research this summer and come up with the findings next fall.
See our Canada category here, and our Health issues category here.
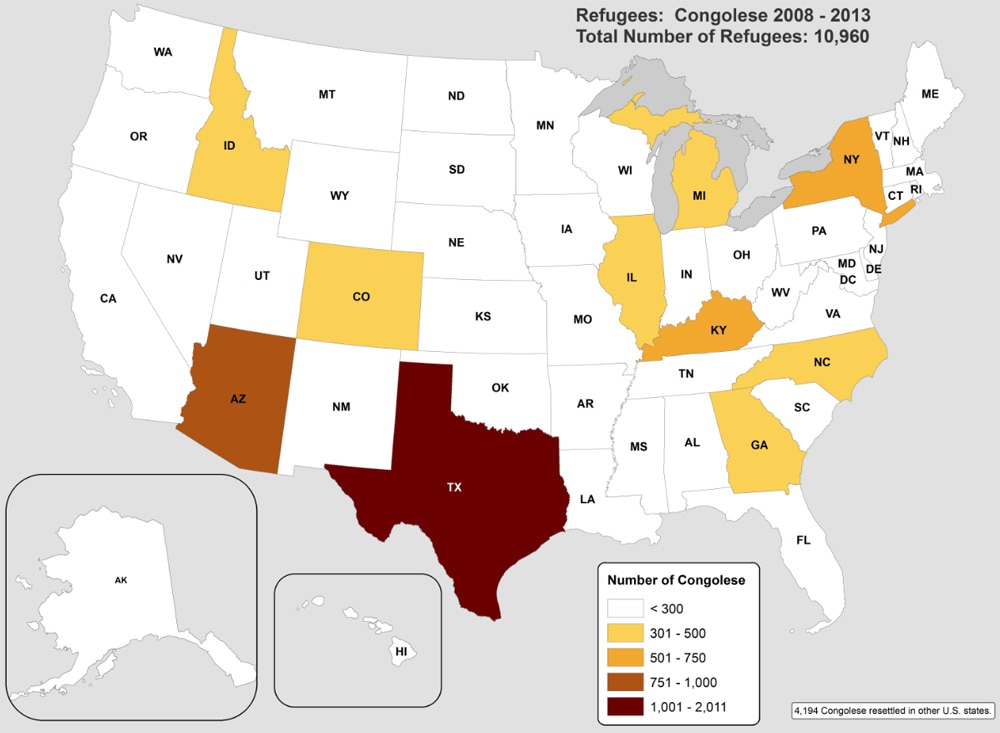
The Centers for Disease Control has some reports you might like to see if Bhutanese and/or Congolese refugees are being resettled in your towns. This could be important information needed by your local health department.
Below is where you can find more information at the CDC website.
The CDC has some great stats, and not just on health issues. http://www.cdc.gov/immigrantrefugeehealth/profiles/congolese/population-movements/index.html
For the Congolese (we have begun the movement of50,000 to the US) the big concerns are parasites, Malaria, and mental health problems relating to sexual and gender-based violence.
Gee, I guess Obamacare’s money tree will be taking care of all these problems! (This post is archived in our ‘health issues’category).
The refugee health profiles found on this page provide key health and cultural information for specific refugee groups resettling to the United States. Information gathered from the World Health Organization (WHO), International Organization for Migration (IOM), the Office of the United Nations High Commissioner for Refugees (UNHCR), US Department of State, and other sources is provided to help resettlement agencies, clinicians, and public health providers facilitate medical screening and interventions appropriate for each refugee group.