Great! More immigrant “entrepreneurs” for ‘Welcoming America’ to brag about!
We just mentioned yesterday in our widely read post on St. Cloud, MN that Somalis are busy setting up ‘home health care’ businesses and we have seen previous news accounts about how easy it is for such businesses to defraud the US taxpayer.
In this DC case, it appears that most of the fraudsters nabbed were from Cameroon according to (not surprisingly!) the last line in the story at CBS.DC. (It is very rare for the nationalities of immigrant law-breakers to be mentioned at all, so for this we are grateful.)
Many of those charged are immigrants from Cameroon in west Africa, but authorities did not go into detail about their nationalities.
Don’t you think there should be a law requiring that the public be informed about what LEGAL immigration program allowed these aliens to enter the US in the first place? It is always my first question!
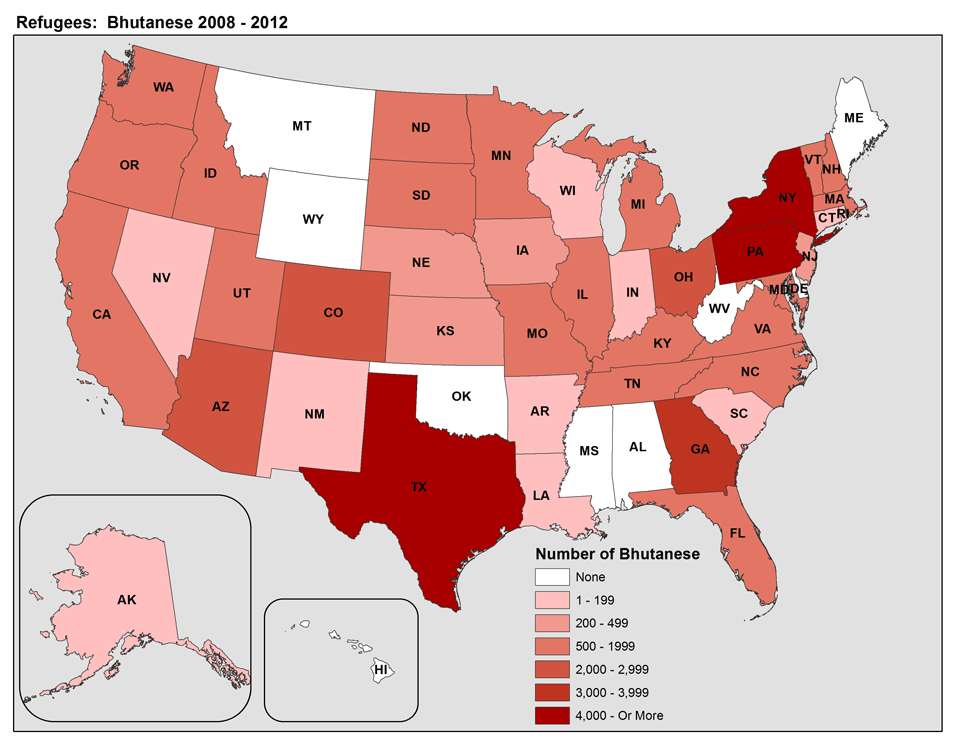
Few of these crooks would be refugees because we don’t take many refugees from Cameroon. Nor does DC resettle many refugees although Maryland surely does. So how did they get here?
From CBS.DC. Hat tip: Bob. Emphasis is mine:
WASHINGTON (CBSDC/AP) — Federal authorities say 25 people have been charged in a wide-ranging scheme to obtain millions of dollars in fraudulent Medicaid payments from the District of Columbia government.
U.S. Attorney Ronald Machen calls it the largest health-care fraud case in the city’s history. It involved bogus claims for home care services, a category of Medicaid claim that has grown dramatically in the city over the past eight years. Machen says fraud is largely responsible for the increase in those claims. The uptick in billings for home care — from $40 million in 2006 to $280 million last year — was part of what tipped off authorities to illegal activity, U.S. Attorney Ronald Machen said.
“We concluded that much of the growth was due to aggressive networks of fraudsters paying kickbacks to beneficiaries to manufacture false claims for nonexistent services,” Machen said, later adding: “Medicaid fraud in the District of Columbia is at epidemic levels.”

http://www.wjla.com/articles/2014/02/florence-bikundi-arrested-in-medicaid-fraud-crackdown-100429.html
Among those charged Thursday was Florence Bikundi, 51, of Bowie, Md., the owner of a home care agency in suburban Maryland who had lost her nursing license and was ineligible to receive Medicaid payments. Authorities say that by using different names, she was able to bill the city for $75 million in Medicaid payments.
Prosecutors say many of the defendants persuaded patients to fake illness or injury so they could bill Medicaid for home care they didn’t receive. Some of those patients received kickbacks, authorities said, although no patients have been charged.
[….]
Machen said it wasn’t clear whether any of those payments went to legitimate home care services, but Bikundi was able to amass significant personal wealth, authorities said. Among the property seized from her were millions of dollars from 46 bank accounts, a 7,300-square-foot home valued at $927,000 and five luxury vehicles.
Sometimes I think there are fraud training programs abroad before the immigrant even gets here—maybe a Scams 101, or Fraud-planning for Dummies—-because some of the ones we’ve written about on these pages require a level of sophistication and an infusion of seed money that one wouldn’t expect your average migrant to be blessed with.
Just a reminder! We are posting stories like this one at a new facebook page entitled ‘Diversity’s Dark Side.’ Check it out and “Like” it, here.